
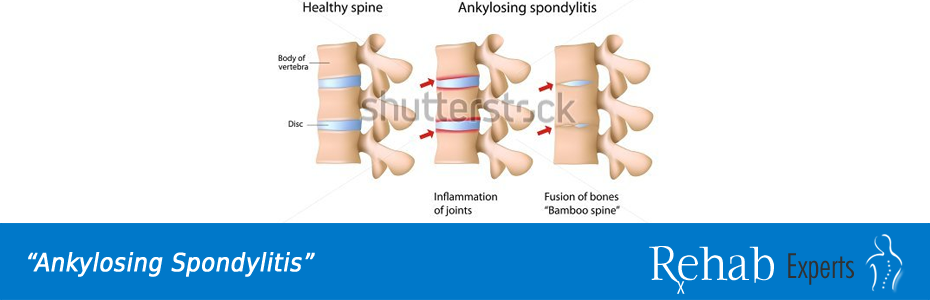
The term ankylosing spondylitis (AS) is not necessarily ideal for this disease, as only a small minority of patients progress to a bent, fused spine. Ankylosing spondylitis is a chronic disorder of the spine and sacroiliac joints, in which inflammatory lesions are associated with progressive stiffening of the spine and radiological calcification of spinal ligaments.
Among the most widely accepted criteria for diagnosis of AS are those developed in Rome (1961) and New York (1996). The most common way to satisfy the criteria is radiological evidence of grade III or IV bilateral sacroiliitis together with a history of pain and/or limitation of motion. The presence or absence of the HLA-B27 antigen does not alone confirm the diagnosis. This disease is almost always diagnosed by means of a radiological examination confirming sacroilitis. Therefore, a patient with symptomatic sacroiliitis, though lacking the HLA-B27 antigen, may still have AS.
Clinical Features
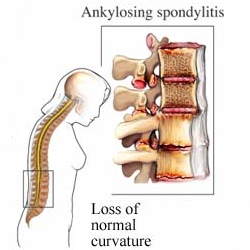
Common symptoms include a gradual onset of low back pain, usually worse in the evening. Morning stiffness is common; activity usually decreases the discomfort. In established cases, spinal mobility and chest expansion are reduced. Various sacroiliac “stress test” are not reliable clinical indicators. Progressive postural changes, such as forward stoop, are associated with tightness of heel cords, hamstrings, fleors, and pectorals. Some conditions associated with AS include ulcerative colitis, psoriasis, urethritis, iritis, aortic incompetence, and cardiac conduction defects.
Management
Comprehensive physiatric management includes use of medication, physical therapy, and patient education.
Medication
Indomethacin (Indocin) (up to 200mg/daily) and phenylbutazone (up to 400 mg/daily) are currently recommended drugs of choice. Try other NSAIDs if these are not tolerated.
Physical Therapy
The objectives of physical therapy in treatment of AS are to maintain normal spinal column position, strengthen spinal muscles, increase breathing capacity, maintain joint mobility, and relieve symptoms. Exercise include deep breathing, back extension and strengthening, stretching of pectorals, hip flexors, hamstrings, and heel cords; trunk mobility; and neck and shoulder mobility. Modalities may be employed as needed.
Patient ducation
An education program includes a description of the disease and its course, with a rationale of needed exercises and development of posture consciousness. The need for adequate rest should be stressed, and the use of proper sleeping surfaces, including a hard mattress with few, if any, pillows. Advie the patient to avoid undesirable physical activities such as body contact sports.
Outcome
The prognosis of AS is usually better than that of rheumatoid arthritis, in that only a minority of patients ultimately develop a significant disabling spinal deformity. Progressive disease is less common in women.
[tagline_box link=”http://www.rehabexperts.com.ph/contact-us” linktarget=”” button=”Contact us now!” title=”Physical Therapy Home Service” description=”Are you a person suffering from some physical disabilities? Do you intend to find a solution to your physical disabilities? Are you already tired masking the pain and intend to find a solution to your physical disabilities? Do you intend to address the root-cause of pain and find a lasting remedy to your physical disabilities? Are you looking for a good quality physical therapy home service?”][/tagline_box]

Resources:
[one_half last=”no”]
[/one_half]